
VASCULAR LESIONS
CEREBRAL ANEURYSMS
Brain aneurysm can exist 1-2% of the population. For the most part, they are quiet and do no produce symptoms until they rupture. When they rupture, they produce a subarachnoid hemorrhage and this in turn can be fatal in 40% of cases. The classic presentation is described as "the worst headache of my life." Approximately 15% of patients with aneurysmal subarachnoid hemorrhage die before making to the hospital. There is a good majority of survivors that are left with significant morbidity and experience permanent neurological deficits. Some patients may require some form of life support. Although aneurysmal rupture can be fatal, certain characteristics of the aneurysm related to the morphology can suggest a higher rupture risk. There is a correlation between the size of the aneurysm and the rupture risk as shown by the International Study of Unruptured Intracranial Aneurysms. Multiple aneurysms can also suggest a higher rupture risk. Other factors in which found be taken into consideration for treatment include female smokers, genetic disorders associated with aneurysm rupture, family history of aneurysm rupture, and psychological intolerance. There are risks that go along with treatment of cerebral aneurysms and not all cases of unruptured aneurysms are going to require treatment. When treatment is warranted, surgical clipping and minimally invasive coiling procedures can be used to treat aneurysms. A multitude of factors play into deciding who would be a candidate for surgery versus coiling of an aneurysm. Below are angiograms showing the vasculature of the brain before and after surgical clipping of aneurysms.
Brain aneurysm can exist 1-2% of the population. For the most part, they are quiet and do no produce symptoms until they rupture. When they rupture, they produce a subarachnoid hemorrhage and this in turn can be fatal in 40% of cases. The classic presentation is described as "the worst headache of my life." Approximately 15% of patients with aneurysmal subarachnoid hemorrhage die before making to the hospital. There is a good majority of survivors that are left with significant morbidity and experience permanent neurological deficits. Some patients may require some form of life support. Although aneurysmal rupture can be fatal, certain characteristics of the aneurysm related to the morphology can suggest a higher rupture risk. There is a correlation between the size of the aneurysm and the rupture risk as shown by the International Study of Unruptured Intracranial Aneurysms. Multiple aneurysms can also suggest a higher rupture risk. Other factors in which found be taken into consideration for treatment include female smokers, genetic disorders associated with aneurysm rupture, family history of aneurysm rupture, and psychological intolerance. There are risks that go along with treatment of cerebral aneurysms and not all cases of unruptured aneurysms are going to require treatment. When treatment is warranted, surgical clipping and minimally invasive coiling procedures can be used to treat aneurysms. A multitude of factors play into deciding who would be a candidate for surgery versus coiling of an aneurysm. Below are angiograms showing the vasculature of the brain before and after surgical clipping of aneurysms.

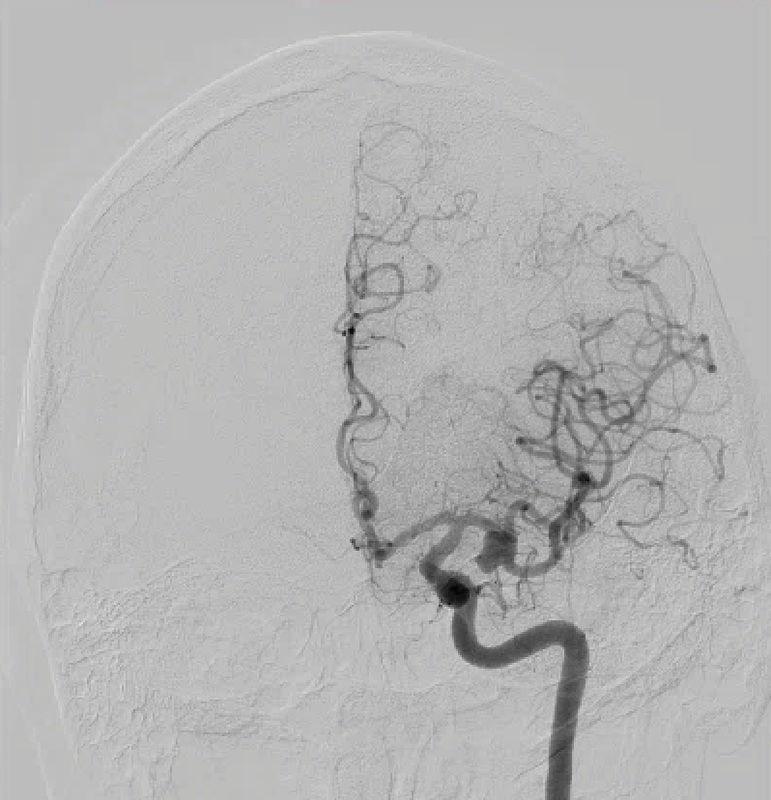
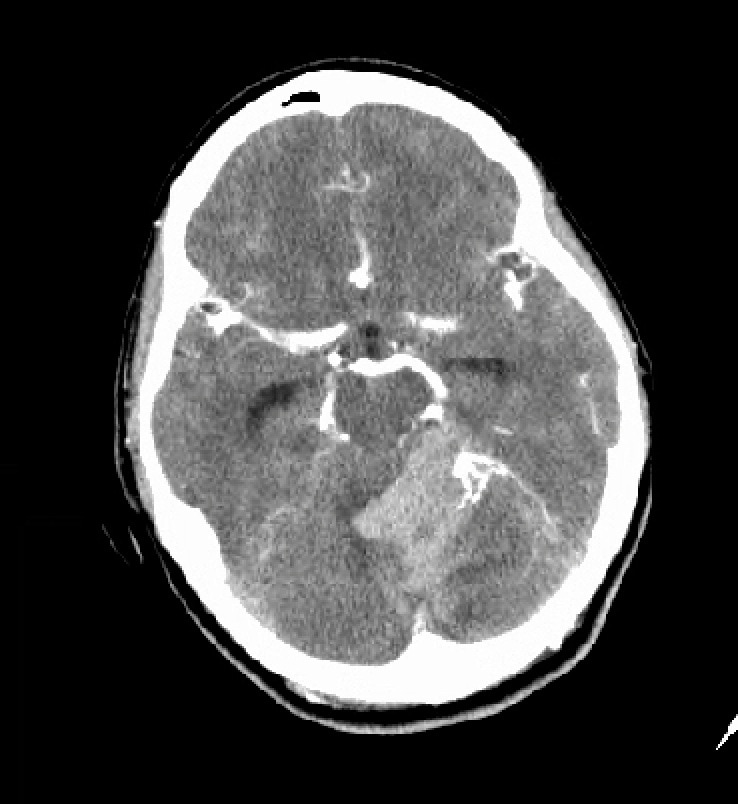
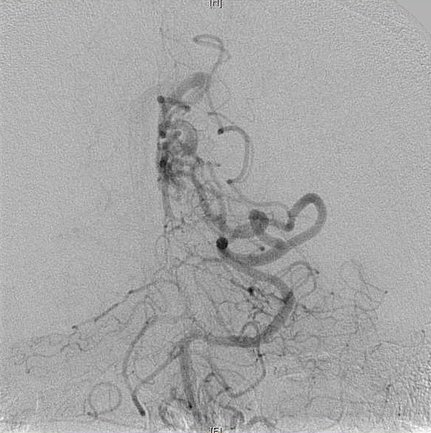
This is a 56 year old male who presented to the emergency room with a sudden onset of headaches. He was found on a CAT scan to have diffuse subarachnoid hemorrohage. Work up with an angiogram shows middle cerebral artery aneurysms on both sides of his brain.

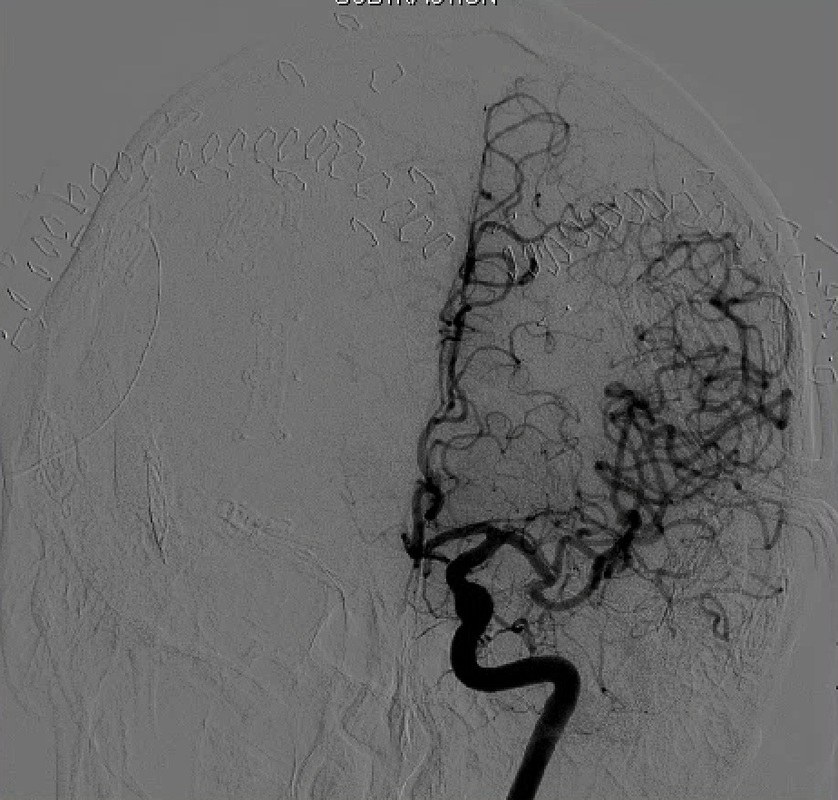
Both aneurysms were treated surgically successfully without injuring any of the vessels supplying the brain.

This is large posterior communicating artery aneurysm.
|
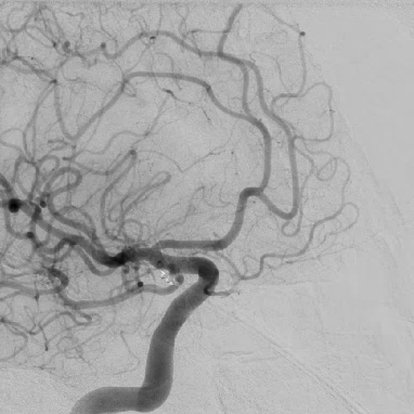
This aneurysm underwent surgically clipping and a post-operative angiogram showed patency of all the vessels with obliteration of the aneurysm.
|
ARTERIOVENOUS MALFORMATIONS
Like aneurysms, arteriovenous malformations (AVMs) can produce hemorrhage in the brain. They can produce bleeding into the brain parenchyma itself and may required emergent surgical intervention to remove to blood clot. Unlike an aneurysm which needs to be secured within 24-48 hours after a rupture has occurred, AVMs can be treated in a delayed fashion if the patient is stable and the hemorrhage is small. The size and location can dictate how risky it can be to treat. AVMs located near important structures (such as speech or motor strength) or in deeper locations can make removing the AVM difficult. Multiple modalities can be used to treat AVMs: 1) surgical intervention 2) embolization 3) radiosurgery. Rarely can an AVM be cured with intraarterial embolization alone. It can take up to two years to see a treatment response to the radiosurgery. Thus, the treatment of each AVM is individualized. The rupture risk of an AVM has approximately 4% per year.
Like aneurysms, arteriovenous malformations (AVMs) can produce hemorrhage in the brain. They can produce bleeding into the brain parenchyma itself and may required emergent surgical intervention to remove to blood clot. Unlike an aneurysm which needs to be secured within 24-48 hours after a rupture has occurred, AVMs can be treated in a delayed fashion if the patient is stable and the hemorrhage is small. The size and location can dictate how risky it can be to treat. AVMs located near important structures (such as speech or motor strength) or in deeper locations can make removing the AVM difficult. Multiple modalities can be used to treat AVMs: 1) surgical intervention 2) embolization 3) radiosurgery. Rarely can an AVM be cured with intraarterial embolization alone. It can take up to two years to see a treatment response to the radiosurgery. Thus, the treatment of each AVM is individualized. The rupture risk of an AVM has approximately 4% per year.
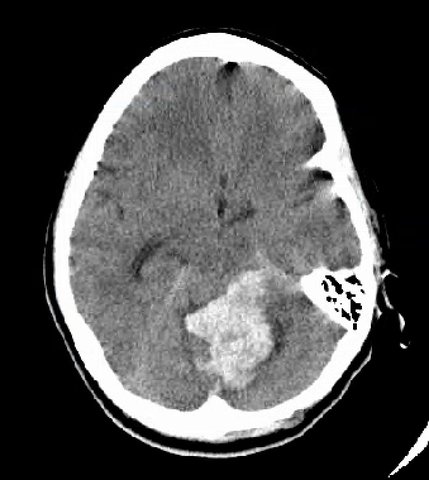
Head CT showing a large bleed in the cerebellum
|
CT angiogram showing evidence of an arteriovenous malformation in the cerebellum.
|
Left occipital AVM: Pre-op
|

Left occipital AVM: Post-op
|
TRIGEMINAL NEURALGIA/HEMIFACIAL SPASM
In the brain, there can be abnormal compression of cranial nerves by arteries or veins. When this occurs, patients can either suffer from a condition known as trigeminal neuralgia or hemifacial spasm. Trigeminal neuralgia produces lancinating pain in the face and can be set off by predictable causes (such as chewing, brushing teeth, etc.). In the past before treatment was available, it was known as "the suicide disease" because the pain could be intense. Medications to treat trigeminal neuralgia is the first line of treatment. When medications fail, then surgery is an option. Surgery is performed to create a barrier between the blood vessel and the trigeminal nerve, Results are encouraging showing 98% initial pain relief and 70% pain free at 10 years after the operation (Taha JM, Tew JM Jr: Comparison of surgical treatments for trigeminal neuralgia: Reevaluation of radiofrequency rhizotomy. Neurosurgery 38:865-871, 1996)
In the brain, there can be abnormal compression of cranial nerves by arteries or veins. When this occurs, patients can either suffer from a condition known as trigeminal neuralgia or hemifacial spasm. Trigeminal neuralgia produces lancinating pain in the face and can be set off by predictable causes (such as chewing, brushing teeth, etc.). In the past before treatment was available, it was known as "the suicide disease" because the pain could be intense. Medications to treat trigeminal neuralgia is the first line of treatment. When medications fail, then surgery is an option. Surgery is performed to create a barrier between the blood vessel and the trigeminal nerve, Results are encouraging showing 98% initial pain relief and 70% pain free at 10 years after the operation (Taha JM, Tew JM Jr: Comparison of surgical treatments for trigeminal neuralgia: Reevaluation of radiofrequency rhizotomy. Neurosurgery 38:865-871, 1996)
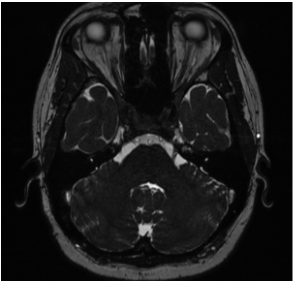
MRI FIESTA Study showing the superior cerebellar artery contacting the trigeminal nerve
|
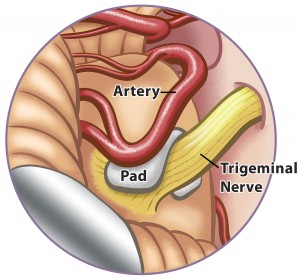
Diagram showing the placement of a Teflon wedge between the trigeminal nerve and the superior cerebellar artery
|
Other procedures to treat trigeminal neuralgia are available and are know as ablative procedures. There procedures destroy nerve cells and produce numbness to reduce or eliminate the pain. The two options here are stereotactic radiation and percutaneous ablation. Stereotactic radiation uses a high single one time dose of radiation focused at the trigeminal nerve. Percutanous technique entail using a needle that is aimed at the trigeminal nerve through the base of the skull and using either radiofrequency, balloon compression, or alcohol injection to destroy the nerve cells.
Like trigeminal neuralgia, hemifacial spasm is caused by compression of the facial nerve by an artery inside the skull. The can cause disfigurement of the face and social embarrassment. The treatment is similar to treatment for trigeminal neuralgia: the creation of a barrier between the nerve and artery.
Like trigeminal neuralgia, hemifacial spasm is caused by compression of the facial nerve by an artery inside the skull. The can cause disfigurement of the face and social embarrassment. The treatment is similar to treatment for trigeminal neuralgia: the creation of a barrier between the nerve and artery.
BRAIN TUMORS
PRIMARY BRAIN NEOPLASMS
Tumors that originate from the brain itself can present with headaches, seizures, speech difficulties, weakness, vision loss, or lethargy. When there is a tumor seen on imaging, we evaluate the location of the lesion and assess whether it is feasible to resect the tumor without causing neurological deficits. If the MRI suggest a high grade tumor, the goals of surgery are then to 1) obtain tissue diagnosis 2) reduce the mass of effect of the lesion on the surrounding structures 3) debulk as much tumor as possible without producing neurological deficits. Every surgeon should utilize caution in taking out tumors. A more aggressive resection does not always imply a better prognosis. Furthermore, each patient have their own goals in terms of treatment which can also include radiation or chemotherapy.
Tumors that originate from the brain itself can present with headaches, seizures, speech difficulties, weakness, vision loss, or lethargy. When there is a tumor seen on imaging, we evaluate the location of the lesion and assess whether it is feasible to resect the tumor without causing neurological deficits. If the MRI suggest a high grade tumor, the goals of surgery are then to 1) obtain tissue diagnosis 2) reduce the mass of effect of the lesion on the surrounding structures 3) debulk as much tumor as possible without producing neurological deficits. Every surgeon should utilize caution in taking out tumors. A more aggressive resection does not always imply a better prognosis. Furthermore, each patient have their own goals in terms of treatment which can also include radiation or chemotherapy.
PRE-OP
|
3 YEAR POST-OP
|
MENINGIOMAS
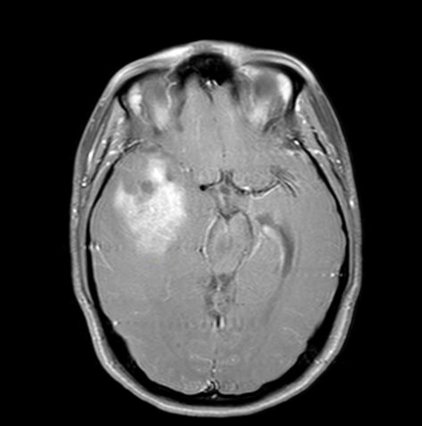
Meningiomas are common benign tumors that are outside of the brain and originate from the tissue covering the brain. Smaller lesions usually require no treatment unless they enlarge. Larger lesions such as the one pictured can cause pressure on the surrounding structured and cause loss of neurological function. In these cases, surgical intervention is warranted. Since these tumors are usually separate (but can be adherent) to the surrounding brain, they are able to be completely resected in the majority of cases with minimal disruption of the brain. Thus the outcomes are favorable.
Meningiomas are common benign tumors that are outside of the brain and originate from the tissue covering the brain. Smaller lesions usually require no treatment unless they enlarge. Larger lesions such as the one pictured can cause pressure on the surrounding structured and cause loss of neurological function. In these cases, surgical intervention is warranted. Since these tumors are usually separate (but can be adherent) to the surrounding brain, they are able to be completely resected in the majority of cases with minimal disruption of the brain. Thus the outcomes are favorable.
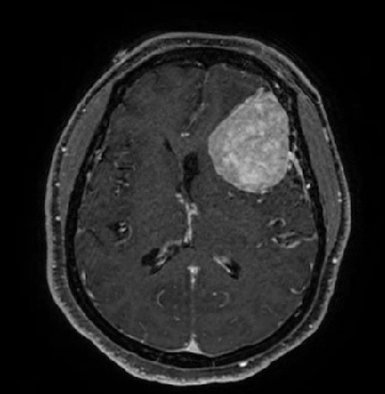
PRE-OP
|
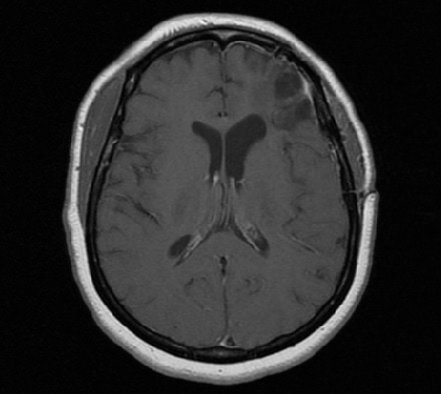
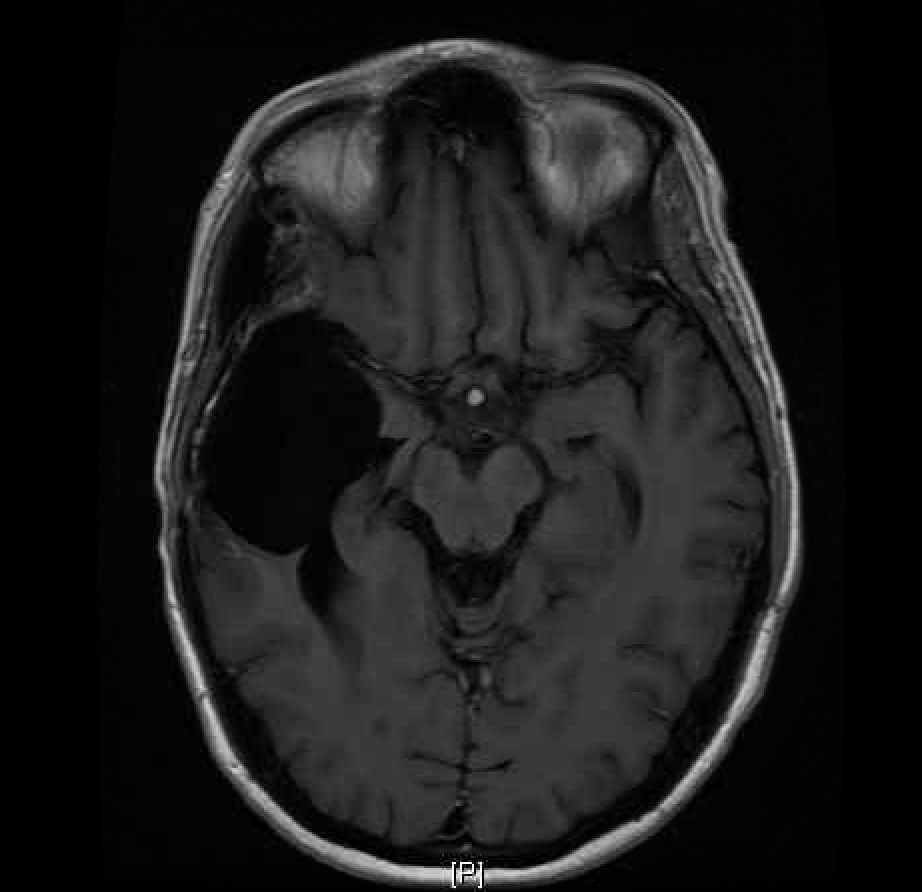
1 YEAR POST-OP
|
PITUITARY TUMORS
Pituitary adenomas are benign tumors that are located behind your nose. It is located in a region between your two carotid arteries and below the optic nerve (responsible for vision) at the base of the skull.. As they enlarge, they can place pressure on the optic nerve and this can lead to vision loss. Thus, in every case, it is important to determine if visual deficits are present. An ophthalmologist is able to perform a visual field test to look for these deficits. It is also important to look for abnormalities in your hormones levels. A subtype of pituitary adenomas known as prolactinomas can be treated successfully with medication thus alleviating the need for surgery. Some abnormal secreting pituitary adenomas can secrete growth hormone or promotes the secretion of steroids thus altering the appearance of the individual. In these circumstances, surgery is recommended regardless of the size of the lesion. Surgery of the pituitary gland has been present since the late 1800s and has been refined since that time. The creation of antibiotics, x-ray, operating microscope and the endoscope has led to the successful treatment of pituitary tumors through the nose.
Pituitary adenomas are benign tumors that are located behind your nose. It is located in a region between your two carotid arteries and below the optic nerve (responsible for vision) at the base of the skull.. As they enlarge, they can place pressure on the optic nerve and this can lead to vision loss. Thus, in every case, it is important to determine if visual deficits are present. An ophthalmologist is able to perform a visual field test to look for these deficits. It is also important to look for abnormalities in your hormones levels. A subtype of pituitary adenomas known as prolactinomas can be treated successfully with medication thus alleviating the need for surgery. Some abnormal secreting pituitary adenomas can secrete growth hormone or promotes the secretion of steroids thus altering the appearance of the individual. In these circumstances, surgery is recommended regardless of the size of the lesion. Surgery of the pituitary gland has been present since the late 1800s and has been refined since that time. The creation of antibiotics, x-ray, operating microscope and the endoscope has led to the successful treatment of pituitary tumors through the nose.
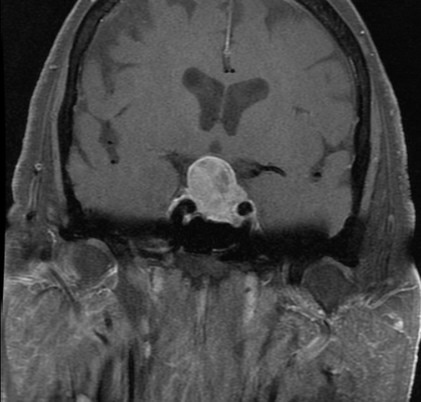
PRE-OP
|
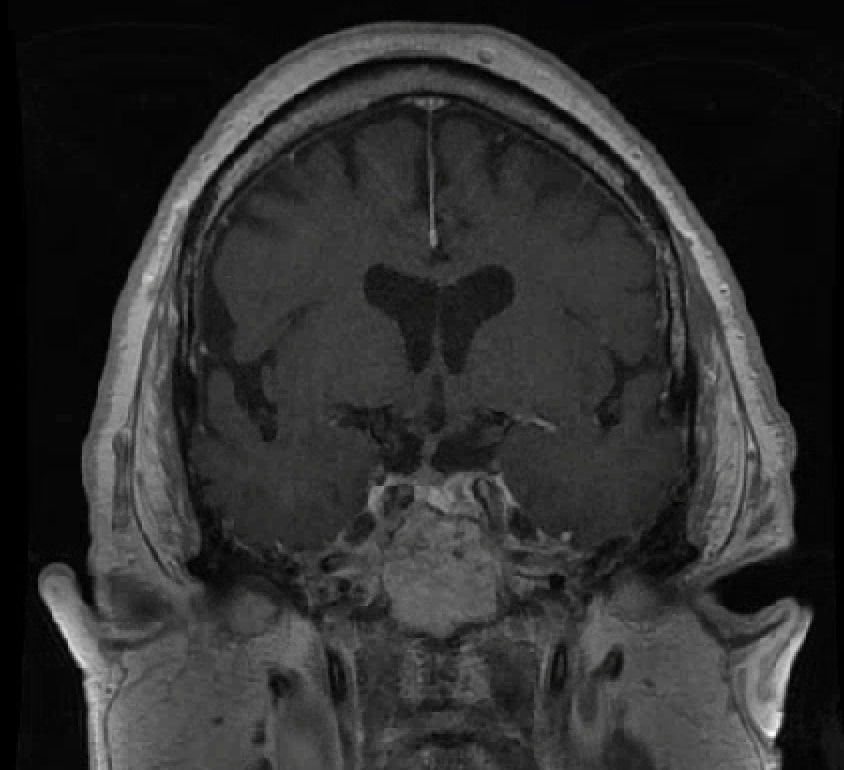
1 YEAR POST-OP
|
